




























The human body is a marvel. It functions harmoniously when cells, tissues, and organs collectively do their part in sustaining their micro- and macro-systems. Systems unsurprisingly have finely-tuned degrees of tolerance; once there is dysregulation beyond natural correction, whether because of a lack of control or a process insufficiency, disease wrecks this marvelous body.
This simple concept extends into the regulation of its bodily byproducts that maintains homeostasis. Many might immediately think of metabolic waste in its form that is excreted and relatively easily collected, such as feces, urine, sweat, etc. Within the confines of the body itself, however, there can be other improper collections of physical byproducts, including the dreaded stones. The kidney stones, bladder stones, gall stones, tonsil stones, bezoars; within the large grouping of urinary system stones, the calcium oxalate, uric, cystine, staghorn stones affect the selected in the population, the stone formers1,2.
Disease researchers in the field of nephrology and urology are working to better understand the molecular mechanisms involved in kidney stone disease (KSD) progression, focusing on insights into cause and effect and notes on prevention or health promotion. The field continues to leverage developments in precision medicine, genetic risk factors, lifestyles, and the likes1. But it doesn't, nor should it, stop there. After the seeding and unchecked growth of these kidney stones have reached a point where passing may be unlikely even with shock wave lithotripsy (SWL) or with too high a risk of injury, one of the possible next options may involve physical removal via ureteroscopy (URS) or a more aggressive percutaneous nephrolithotomy (PCNL)2, among other options.
There are several reports on HAIs (hospital-acquired infections) generally, of its most prevalent types, and of AMRs (antimicrobial resistance) that are adding to the conversations about global burden and surveyed consequences. The microbe-enthused researchers are hard at work in that space as well. And, in recent years, when it comes to PCNL, the European Association of Urology (EUA) has updated their urological guidelines that includes a strong recommendation for the collection of urine or stone culture directly from the renal pelvis during PCNL, actioning on their evidence-based approach to help counter risks of SIRS (systemic inflammatory response syndrome) and sepsis2.
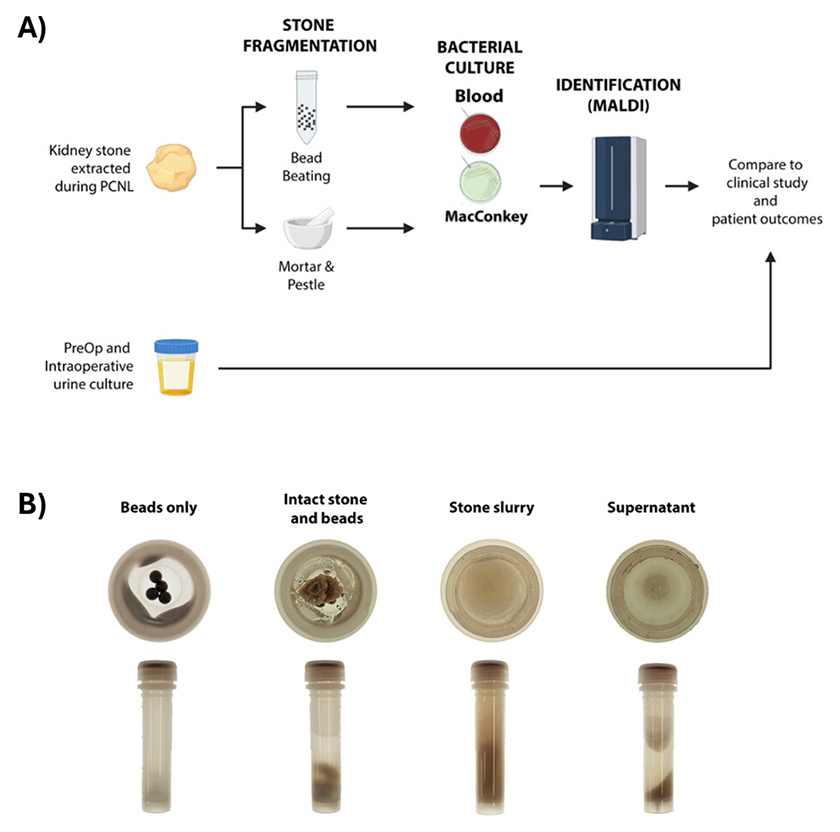
Fig 1: Study design. The study design is outlined in (A). Specimens are processed by BB or MP and then plated. Isolated colonies are identified by MALDI-TOF MS and compared to preoperative urine cultures. Examples of bead tubes pre-processing and post-processing are shown in (B). [Taken and used, without any adaptation or changes, directly from On, T. A., Anwar, F., Chien, A. L., Hsu, C.-H., Vedantam, G., Lainhart, W. D., & Tzou, D.T. (2025). Bead beating demonstrates enhanced bacterial detection in kidney stone culture compared to traditional mortar-pestle processing. Microbiology spectrum, 13(8), e0088925. https://doi.org/10.1128/spectrum.00889-25] 3
Though collecting rocks and stones may not be what first comes to mind within biological sciences, they are valuable biospecimens that live in biospecimen cores, biorepositories, and biobanks; they are actively being leveraged at length by researchers within their consortiums and networks, including the NIH-driven rare kidney stone consortium (RKSC) and the NIDDK-funded urinary stone disease research network (USDRN) for a variety of multiomics research work. As with single-site, local, or global cross-site collaborations, standardization of sample prep are thought to be critical to derive evidence-based insights.
Additionally, for matrices like these that are variable in nature, the extra effort in reducing process variability in the early analytical steps may impact downstream data outputs, including successful detection of infectious organisms from culture. Automation-enabled solutions such as bead-beating could additively help with both streamlining early prep processes before research samples enter complex analytical assays for biomarkers or for bacterial culturing, detection, and identification of micro-organisms3.
To see their research protocol and data, read this open access article from the team at the University of Arizona, “Bead beating demonstrates enhanced bacterial detection in kidney stone culture compared to traditional mortar-pestle processing”3, highlighting bead-beating on a bead mill homogenizer as a more sensitive stone culture protocol for detecting bacteria within kidney stones compared to traditional techniques, such as mortar and pestle, in their study.
Reference
- Shastri, S., Patel, J., Sambandam, K. K., & Lederer, E. D. (2023). Kidney Stone Pathophysiology, Evaluation and Management: Core Curriculum 2023. American journal of kidney diseases : the official journal of the National Kidney Foundation, 82(5), 617–634. https://doi.org/10.1053/j.ajkd.2023.03.017
- Akram, M., Jahrreiss, V., Skolarikos, A., Geraghty, R., Tzelves, L., Emilliani, E., Davis, N. F., & Somani, B. K. (2024). Urological Guidelines for Kidney Stones: Overview and Comprehensive Update. Journal of clinical medicine, 13(4), 1114. https://doi.org/10.3390/jcm13041114
- On, T. A., Anwar, F., Chien, A. L., Hsu, C.-H., Vedantam, G., Lainhart, W. D., & Tzou, D. T. (2025). Bead beating demonstrates enhanced bacterial detection in kidney stone culture compared to traditional mortar-pestle processing. Microbiology spectrum, 13(8), e0088925. https://doi.org/10.1128/spectrum.00889-25
For research use only. Not for diagnostic procedures.



